Carpal tunnel syndrome (CTS) is the most commonly diagnosed and treated entrapment neuropathy. The syndrome is characterized by pain, paresthesia, and weakness in the median nerve distribution of the hand. Surgical and nonsurgical treatments exist that can produce excellent outcomes for patients.
An image depicting the carpal canal can be seen below.
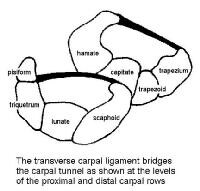 Cross sections of the carpal canal at the levels of the proximal and distal carpal rows are depicted. The transverse carpal ligament bridges the carpal tunnel and is under tension.
Cross sections of the carpal canal at the levels of the proximal and distal carpal rows are depicted. The transverse carpal ligament bridges the carpal tunnel and is under tension. American Academy of Orthopaedic Surgeons guidelines
The AAOS has developed the following clinical guidelines for the treatment of carpal tunnel syndrome (level of evidence provided in parentheses):[1]Recommendation 1
A course of nonoperative treatment is an option in patients diagnosed with carpal tunnel syndrome (CTS). Early surgery is an option when there is clinical evidence of median nerve denervation or the patient elects to proceed directly to surgical treatment. (Grade C, level V)
Recommendation 2
We suggest another nonoperative treatment or surgery when the current treatment fails to resolve the symptoms within 2-7 weeks. (Grade B, level I and II)
Recommendation 3
We do not have sufficient evidence to provide specific treatment recommendations for carpal tunnel syndrome when found in association with the following conditions: diabetes mellitus, coexistent cervical radiculopathy, hypothyroidism, polyneuropathy, pregnancy, rheumatoid arthritis, and carpal tunnel syndrome in the workplace. (Inconclusive, No evidence found)
Recommendation 4a
Local steroid injection or splinting is suggested when treating patients with carpal tunnel syndrome, before considering surgery. (Grade B, level I and II)
Recommendation 4b
Oral steroids or ultrasound are options when treating patients with carpal tunnel syndrome. (Grade C, level II)
Recommendation 4c
We recommend carpal tunnel release as treatment for carpal tunnel syndrome. (Grade A, level I)
Recommendation 4d
Heat therapy is not among the options that should be used to treat patients with carpal tunnel syndrome. (Grade C, level II)
Recommendation 4e
The following treatments carry no recommendation for or against their use: activity modifications, acupuncture, cognitive behavioral therapy, cold laser, diuretics, exercise, electric stimulation, fitness, Graston instrument, iontophoresis, laser, stretching, massage therapy, magnet therapy, manipulation, medications (including anticonvulsants, antidepressants, and nonsteroidal anti-inflammatory drugs [NSAIDs]), nutritional supplements, phonophoresis, smoking cessation, systemic steroid injection, therapeutic touch, vitamin B6 (pyridoxine), weight reduction, yoga. (Inconclusive, level II and V)
Recommendation 5
We recommend surgical treatment of carpal tunnel syndrome by complete division of the flexor retinaculum regardless of the specific surgical technique. (Grade A, level I and II)
Recommendation 6
We suggest that surgeons do not routinely use the following procedures when performing carpal tunnel release: skin nerve preservation (Grade B, level I); epineurotomy (Grade C, level II)
The following procedures carry no recommendation for or against use: flexor retinaculum lengthening, internal neurolysis, tenosynovectomy, ulnar bursa preservation. (Inconclusive, level II and V)
Recommendation 7
The physician has the option of prescribing preoperative antibiotics for carpal tunnel surgery. (Grade C, level III)
Recommendation 8
We suggest that the wrist not be immobilized postoperatively after routine carpal tunnel surgery. (Grade B, level II)
We make no recommendation for or against the use of postoperative rehabilitation. (Inconclusive, level II)
Recommendation 9
We suggest physicians use one or more of the following instruments when assessing patients’ responses to CTS treatment for research:
- Boston Carpal Tunnel Questionnaire (disease-specific)
- DASH—Disabilities of the Arm, Shoulder, and Hand (region-specific; upper limb)
- MHQ—Michigan Hand Outcomes Questionnaire (region-specific; hand/wrist)
- Patient Evaluation Measure (region-specific; hand)
- SF-12 or SF-36 Short Form Health Survey (generic; physical health component for global health impact) (Grade B, level I, II, and III)
Recent studies
Jarvik et al compared surgical (57 patients) versus multi-modality, nonsurgical treatment (hand therapy and ultrasound; 59 patients) for carpal tunnel syndrome without denervation. Analyses showed a significant 12-month adjusted advantage for surgery in function and symptoms; there were no clinically important adverse events and no surgical complications. According to the authors, symptoms in both groups improved, but surgical treatment led to better outcome than nonsurgical treatment.[2]In a Mayo Clinic study by Gelfman et al, temporal trends in CTS were assessed for incidence, surgical treatment, and lost time at work. Using Olsmsted County residents as the study population, 10,069 residents were found to have been diagnosed with CTS from 1981-2005 (491 per 100,000 person years for women; 258 per 100,000 person years for men; 376 per 100,000 person-years combined). Adjusted annual rates increased from 258 per 100,000 in 1981-1985 to 424 in 2000-2005. The average annual incidence of carpal tunnel release surgery was 109 per 100,000, and that for work-related CTS was 11 per 100,000. According to the authors, the increase seen in this population corresponds to a national epidemic of CTS cases resulting in lost work days that began in the mid-1980s and lasted through the mid-1990s, but the cause for the increase is not yet clear.[3]
Pomerance et al compared direct costs and results for patients with electrodiagnostically proven CTS treated with surgery versus nonsurgical care. In the study, 120 patients were divided into 2 groups: group 1 received nonsurgical therapy, and group 2 received surgical treatment. Follow-up averaged 13 ± 5 months for group 1 and 12 ± 2 months for group 2, with 32 patients in group 1 electing to have surgery during the follow-up period. Cost of care averaged $3,335 ± $2,097 in the nonsurgery group and $3,068 ± $983 in the surgery group. The authors concluded that surgery should be considered as the initial form of treatment when patients are diagnosed with CTS confirmed by nerve conduction studies because surgery provides symptom resolution with a favorable cost analysis.[4]
Wolf et al studied the diagnosis of CTS in the United States military population from 1998-2006 and found the incidence to be 3.98 per 1,000 person-years, which compared with incidences of 1.5 to 3.5 per 1,000 person-years in other regional or working-group populations studied. In the military study, females had a significantly higher incidence of CTS than males, with an adjusted incidence rate ratio of 3.29. CTS incidence was found to increase with age, with the age group 40 years or older having a significantly higher incidence. Additionally, military rank was found to be an independent risk factor for CTS, with rates higher in senior officer and enlisted groups, suggesting that occupational requirements have an effect on CTS within the military.[5]
For excellent patient education resources, visit eMedicine's Hand, Wrist, Elbow, and Shoulder Center and Arthritis Center.
*Some of our clients have suffered impaired hand and forearm trauma due to a serious accident. The Garcia Law Firm, P.C. was able to successfully handle these types of cases. For a free consultation please call us at 1-866- SCAFFOLD or 212-725-1313. edicine's patient education article Carpal Tunnel Syndrome.
No comments:
Post a Comment